Pancreatic Divisum
- Definition: A congenital variation where the dorsal and ventral pancreatic ducts fail to fuse, altering pancreatic juice flow.
- Symptoms: Recurrent upper-abdominal pain, acute or chronic pancreatitis in adulthood.
- Diagnosis: MRCP or secretin-enhanced MRCP confirms ductal anatomy.
- Management: Pain control and enzyme supplementation; endoscopic minor papilla sphincterotomy for drainage; surgery rarely.
- Follow-Up: Monitor for pancreatitis flares and nutritional status.
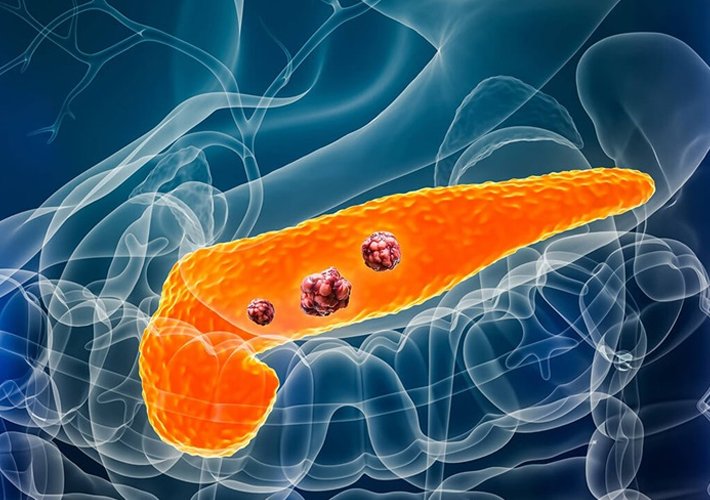
Pancreatic Cystic Neoplasms
- Intraductal Papillary Mucinous Neoplasm (IPMN)
- Mucin-secreting lesion involving main or branch ducts; risk of malignancy.
- Surveillance MRI/EUS; surgical resection if high-risk features (nodules, duct dilation).
• Mucinous Cystic Neoplasm (MCN) - Multiloculated cyst with ovarian-type stroma in body/tail; pre-malignant.
- Early surgical removal; no surveillance if resected.
• Serous Cystic Neoplasm (SCN) - Microcystic, benign lesion often asymptomatic.
- Observation with periodic imaging; resect if symptomatic.
• Solid Pseudopapillary Neoplasm (SPN) - Rare low-grade malignant tumor in young women.
- Complete surgical excision; excellent prognosis.
Pancreatic Neuroendocrine Tumor (PNET)
- Definition: Tumors from islet cells; functional (hormone-secreting) or nonfunctional.
- Symptoms: Insulinoma (hypoglycemia), gastrinoma (ulcers), or nonspecific mass effects.
- Diagnosis: EUS with FNA, somatostatin-receptor imaging, hormone assays.
- Treatment: Surgical resection for localized disease; somatostatin analogs, PRRT, targeted therapy for advanced cases.
Follow-Up: Imaging and hormone levels every 3–6 months