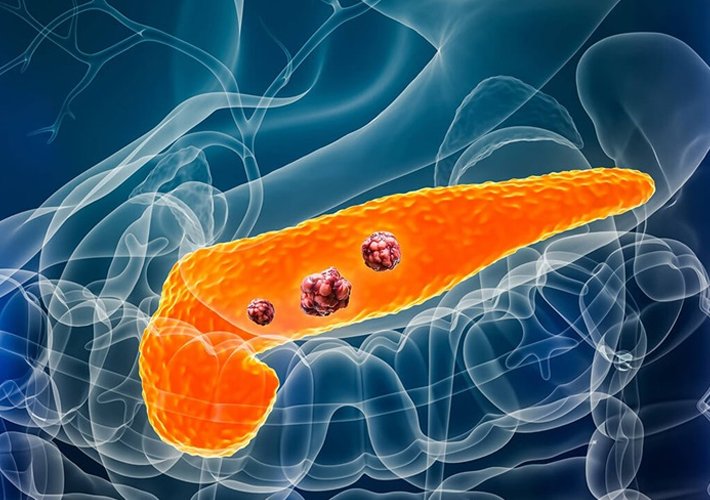
Pancreatic cancer arises from the cells of the pancreas and often presents late with nonspecific symptoms. Early detection and a multidisciplinary treatment approach offer the best outcomes.
Why Do I Need Management?
You may require evaluation and treatment if you have:
- Painless jaundice or dark urine
- Unexplained weight loss and loss of appetite
- Upper abdominal or back pain
- New-onset diabetes or worsening glycemic control
- Imaging (CT/MRI/EUS) showing a pancreatic mass
How Should I Prepare?
- Diagnostic Tests:
- Blood work: liver panel, CA 19-9 tumor marker
- Imaging: contrast-enhanced CT or MRI pancreas protocol
- EUS with fine-needle aspiration (FNA) for tissue diagnosis
- Pre-treatment Assessment:
- Cardio-pulmonary evaluation for fitness for surgery or chemotherapy
- Nutritional assessment; enzyme replacement planning
- Consent & Education:
- Discussion of treatment options, risks, and expected outcomes
- Arrange a family member or friend to accompany you to appointments
What Happens During Treatment?
Treatment is personalized by stage, fitness, and goals:
- Surgical Resection (for resectable tumors)
- Whipple procedure or distal pancreatectomy to remove the tumor with clear margins
- Drain placement for leak monitoring
- Neoadjuvant Therapy (borderline resectable)
- Chemotherapy ± radiation to shrink the tumor before surgery
- Adjuvant Therapy (post-surgery)
- Combination chemotherapy (e.g., FOLFIRINOX or gemcitabine-based) to reduce recurrence risk
- Definitive Chemoradiation (locally advanced, unresectable)
- Concurrent chemotherapy and targeted radiation
- Palliative Care (metastatic disease)
- Systemic chemotherapy regimens
- EUS-guided celiac plexus neurolysis for pain control
- Biliary stenting via ERCP or EUS-BD for jaundice
- Nutritional support with enzyme replacement and specialized diets
What Can I Expect Afterwards?
- Hospital Stay:
- Surgery: 7–14 days depending on procedure and recovery
- Chemotherapy infusions: outpatient or short admission
- Pain & Symptom Management:
- IV and oral analgesics; neurolysis for refractory pain
- Antiemetics to control nausea
- Nutrition:
- Pancreatic enzyme supplements with meals
- Small, frequent, high-protein, high-calorie meals or enteral nutrition
- Activity:
- Early mobilization after surgery
- Gentle activity during chemotherapy; avoid crowds during low blood counts
Risks & Possible Complications
- Surgical: pancreatic fistula (10–20%), delayed gastric emptying (20–30%), bleeding, infection
- Chemotherapy: neutropenia, nausea, fatigue, neuropathy
- Radiation: skin changes, fatigue, GI irritation
- Neurolysis: transient hypotension, diarrhea
- Stenting: occlusion, migration, cholangitis
Seek immediate care if you develop fever, uncontrolled pain, jaundice, severe vomiting, or signs of infection.
Follow-Up
- Surveillance:
- Imaging (CT or MRI) and CA 19-9 every 3 months for 2 years, then every 6 months
- Endocrine and exocrine pancreatic function monitoring
- Supportive Care:
- Ongoing pain and symptom management
- Psychosocial support and palliative care involvement as needed